
What Is the Head Impulse Test (HIT) and What Do the Results Mean?
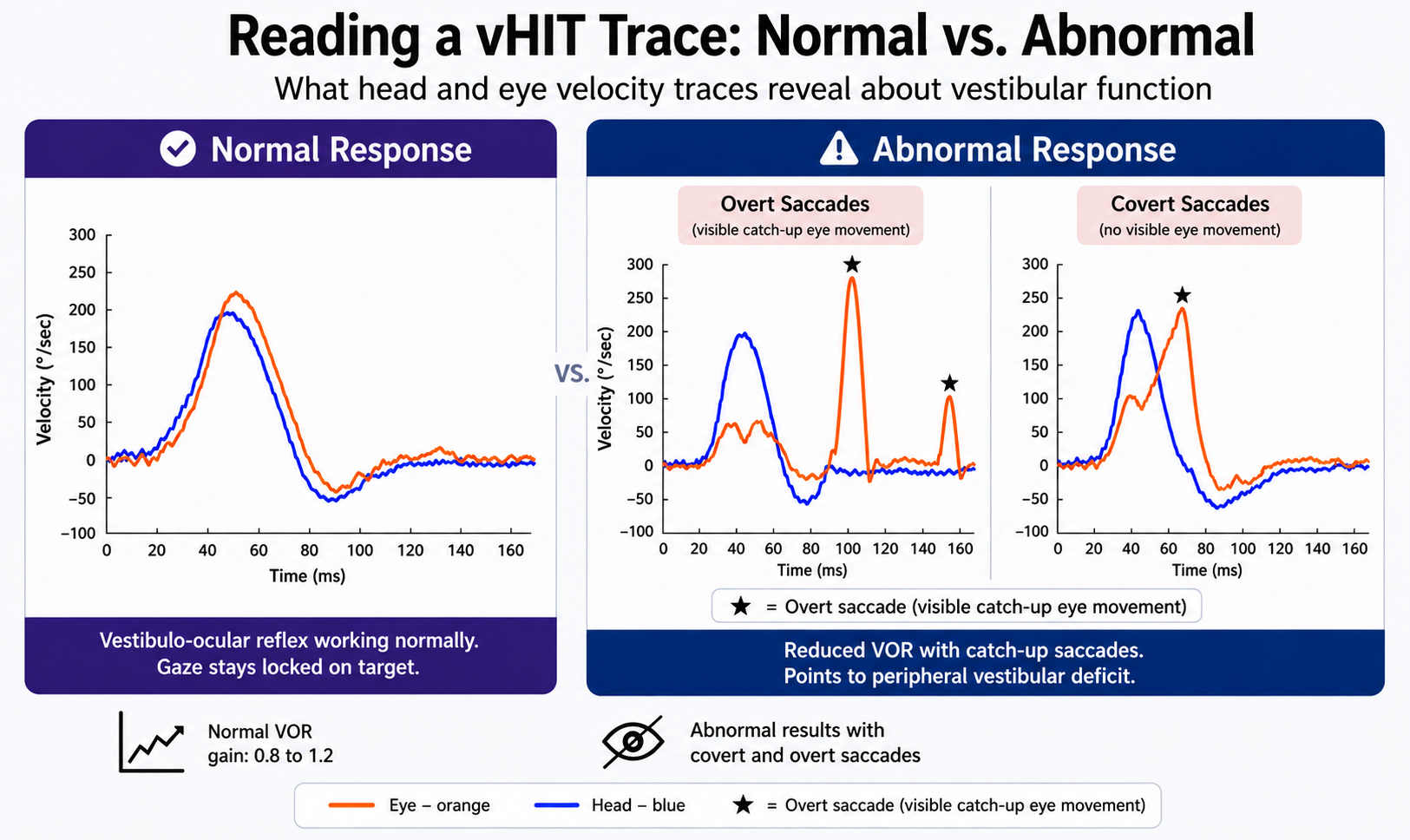
The Short Answer: The head impulse test is a quick clinical test that measures how well the vestibulo-ocular reflex (VOR) works during fast head rotation. Normal results mean the eyes stay locked on a target while the head moves; abnormal results show catch-up saccades, which point to reduced function in one or more semicircular canals.
Dizziness and balance complaints are among the most common reasons patients seek care from ENTs, and neurologists and audiologists,. The head impulse test, first described by Halmagyi GM and Curthoys in 1988, gives clinicians a direct window into the vestibular system.
The head impulse test (HIT) is an exam that evaluates the ability of the vestibular system stabilizing the eye onto a target during fast head movement. The clinician holds the patient’s head, asks them to focus on a target (usually the clinician’s nose), then applies a small, high-acceleration head rotation of about 15 to 20 degrees.
A healthy vestibulo-ocular reflex moves the eyes in the opposite direction at the same speed, keeping gaze locked on the target. If the VOR is weak on one side, the eyes drift with the head and then snap back in a corrective saccade to refind the target.
The test is side-specific. Turning the patient’s head to the right evaluates the right horizontal semicircular canal. Turning it to the left evaluates the left. Vertical planes are tested with diagonal impulses that assess the anterior and posterior canals.
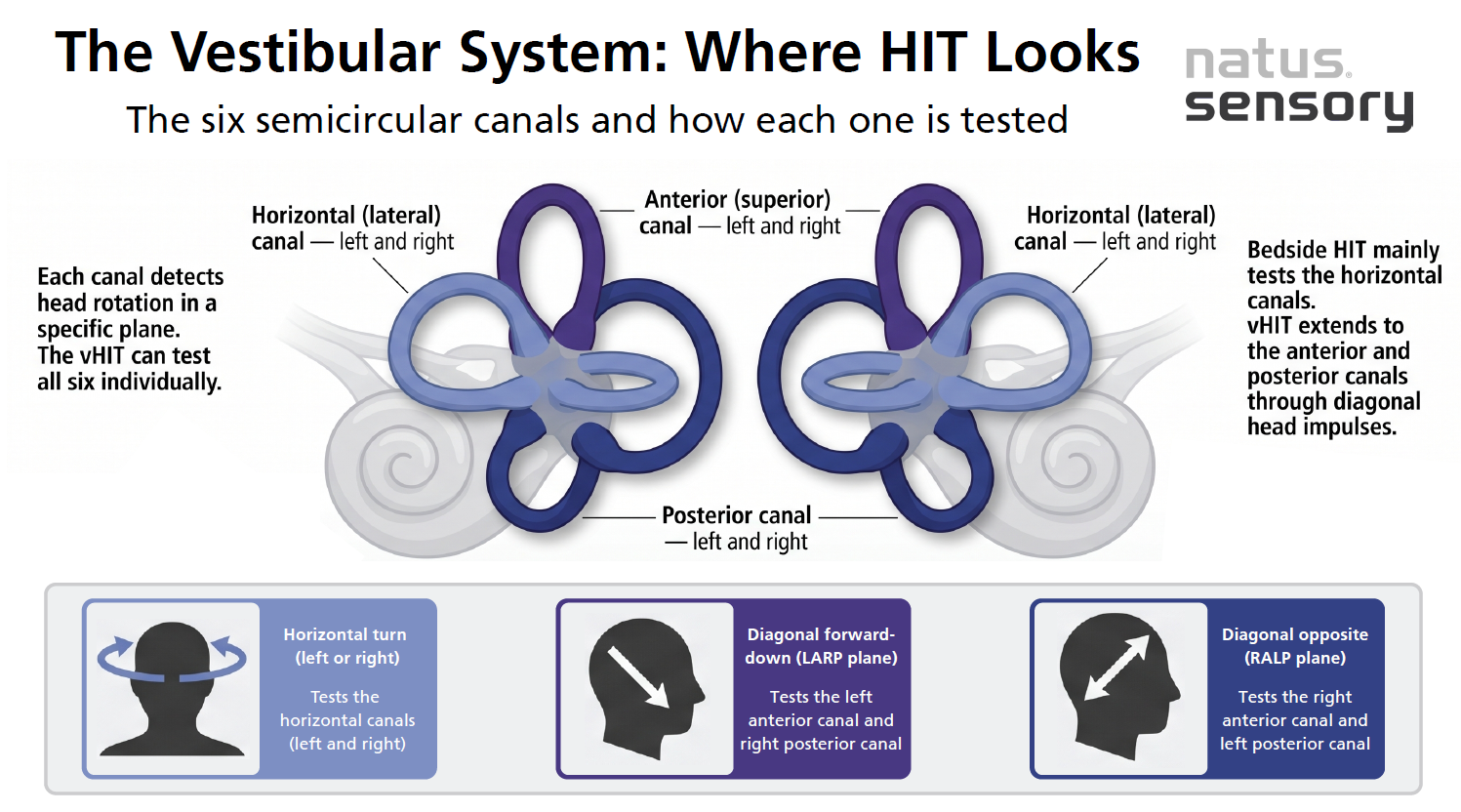
The bedside version of head impulse testing has real limits. The clinician has to spot a catch-up saccade with the naked eye, which only works if the saccade happens after the head stops moving (overt saccades). Fast saccades that happen during head rotation (covert saccades) stay invisible during a bedside exam.
The video head impulse test solves that problem. Lightweight goggles with high-speed cameras record eye velocity and head velocity at high frequency, producing an objective graph of the response. A detailed overview from Halmagyi and colleagues in Frontiers in Neurology walks through how the modern vHIT evolved from the original bedside test.
What are the differences between the two versions?
A landmark study by MacDougall, Weber, McGarvie, Halmagyi GM, and Curthoys in Neurology (2009) compared vHIT with scleral search coils (the reference standard used in vestibular research) in normal subjects and patients with peripheral vestibular deficit. The two methods showed a concordance correlation of 0.930, and vHIT detected both overt and covert saccades as accurately as search coils.
A typical clinical setting for head impulse testing follows this flow:
Impulses need high velocity and high acceleration to activate the high-frequency response of the horizontal canal, matching real-world movements like turning to check traffic.
| Normal Results | Abnormal Results |
For healthy individuals, expect:
A graph from a healthy subject shows the eye velocity trace nearly mirroring the head velocity trace in the opposite direction. |
In a patient with a peripheral vestibular lesion, VOR gain drops below 0.8 and catch-up saccades appear. These corrective saccades come in two types:
|
A study by Blödow and colleagues looked at 117 patients across several peripheral vestibular disorders and found abnormal vHIT results in 94.2% of vestibular neuritis patients. Across the full abnormal cohort, 52% showed both overt catch-up saccades and covert saccades, 34.3% had isolated overt saccades, and 13.7% had only covert saccades. That last group is the one bedside testing routinely misses.
The pattern of abnormality guides the differential diagnosis.
The caloric test irrigates the ear canal with warm or cool water or air, creating a convection current in the lateral semicircular canal that stimulates the VOR. Caloric testing is a low-frequency test, simulating head motion around 0.003 Hz. The video head impulse test operates at high frequency (roughly 2 to 6 Hz), closer to the range of natural head movements. That frequency difference is why the two tests can disagree, and why both still have a place in balance assessment.
Practical differences between the two:
For patients with complex vestibular symptoms, many clinicians run both tests to build a full picture, which normally takes 15 – 20 minutes..
Patients who arrive in the emergency department with sudden vertigo, vomiting, nystagmus, and balance problems fit the definition of acute vestibular syndrome. Both peripheral vestibulopathy (like vestibular neuritis) and posterior circulation stroke can look similar at first glance.
A reduced VOR with catch-up saccades on the affected side points toward a peripheral vestibular lesion. A normal HIT in the same clinical picture raises concern for a central cause. The HINTS exam, developed by Kattah and colleagues, showed that this three-step bedside oculomotor approach was more sensitive than early MRI diffusion-weighted imaging for identifying stroke in acute vestibular syndrome. Because vHIT gives objective data on eye velocity and head velocity, it supports rapid triage in the clinical setting and helps reduce missed stroke diagnoses.

Putting vHIT Results to Work in Your Clinic
The video head impulse test gives clinicians a direct read on how well each semicircular canal is working. A normal result shows the vestibulo-ocular reflex keeping gaze locked during head rotation. An abnormal result, marked by reduced VOR gain and catch-up saccades, points toward peripheral vestibular deficit conditions like vestibular neuritis, bilateral vestibular loss, or ototoxic injury. Video head impulse testing extends that accuracy by capturing covert saccades the naked eye cannot see and providing objective data validated against the gold standard scleral search coils.
Natus Sensory’s ICS® Impulse vHIT, validated against scleral search coils and approved by Drs. Halmagyi and Curthoy, support ENTs, balance specialists and audiologists looking for accurate vestibular testing in everyday practice. To learn more about our balance assessment solutions or the video head impulse test system, contact our team.
Sources:
053412 RevA