
At a Glance: Real ear measurement (REM) is an objective test that measures the actual sound level a hearing aid delivers inside a patient’s ear canal. It allows an audiologist or hearing instrument specialist to verify that amplification levels match prescriptive targets for each individual’s hearing loss and ear canal anatomy.
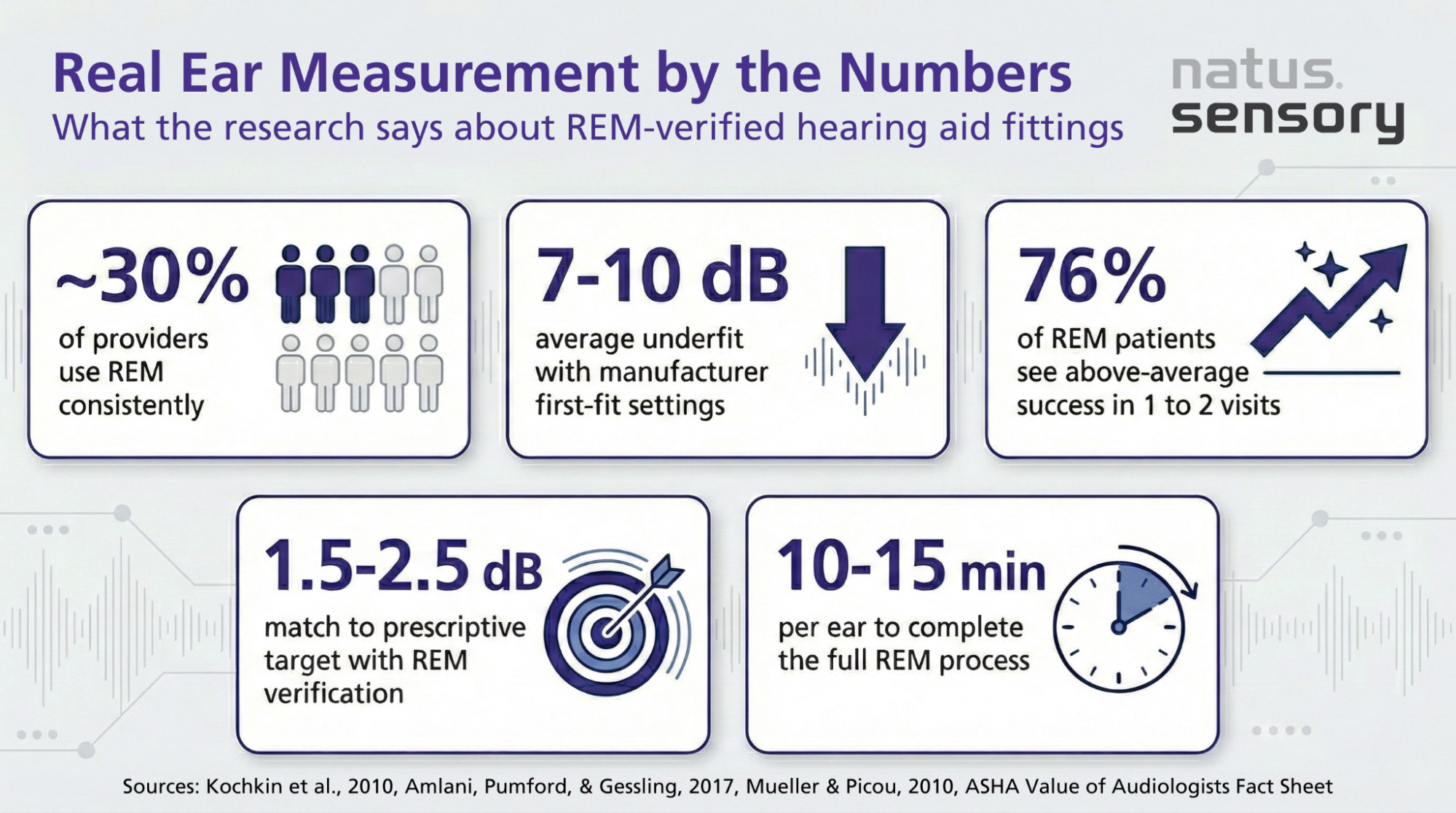
Every person’s ear canal has a unique shape and size, which changes how sound travels and can be perceived. Without real ear verification, hearing aid settings rely on pre-programmed manufacturer defaults designed for typical hearing loss patterns rather than the individual wearer. Both the American Academy of Audiology (AAA) and the American Speech-Language-Hearing Association (ASHA), and in the UK, the British Academy of Audiology (BAA) and British Society of Audiology (BSA) all recommend real ear measurement as the preferred method for verifying hearing aid performance. Yet research suggests that only about 30% of hearing care providers use REM consistently.
Real ear measurement is a precise measurement technique used during a hearing aid fitting. Here’s how it works:
The measurement captures the exact sound level being delivered to the ear, not an estimate. This gives the audiologist objective data to compare the hearing instrument’s output against the prescriptive target set for that patient’s hearing loss.
When a hearing aid is programmed through manufacturer programming software, it uses average ear canal dimensions and generalized algorithms to set initial amplification. This is called a “first fit.” Research published in the Journal of the American Academy of Audiology has shown that first-fit settings commonly underfit by 7 to 10 dB compared to prescriptive targets, particularly in the higher frequencies where speech clarity depends most.
Real ear verification closes that gap. By measuring what’s actually happening inside the patient’s ear canal, clinicians can adjust hearing aid settings until the output matches the prescribed target within 1.5 to 2.5 dB.
The REM process follows a series of steps during the hearing aid fitting appointment.
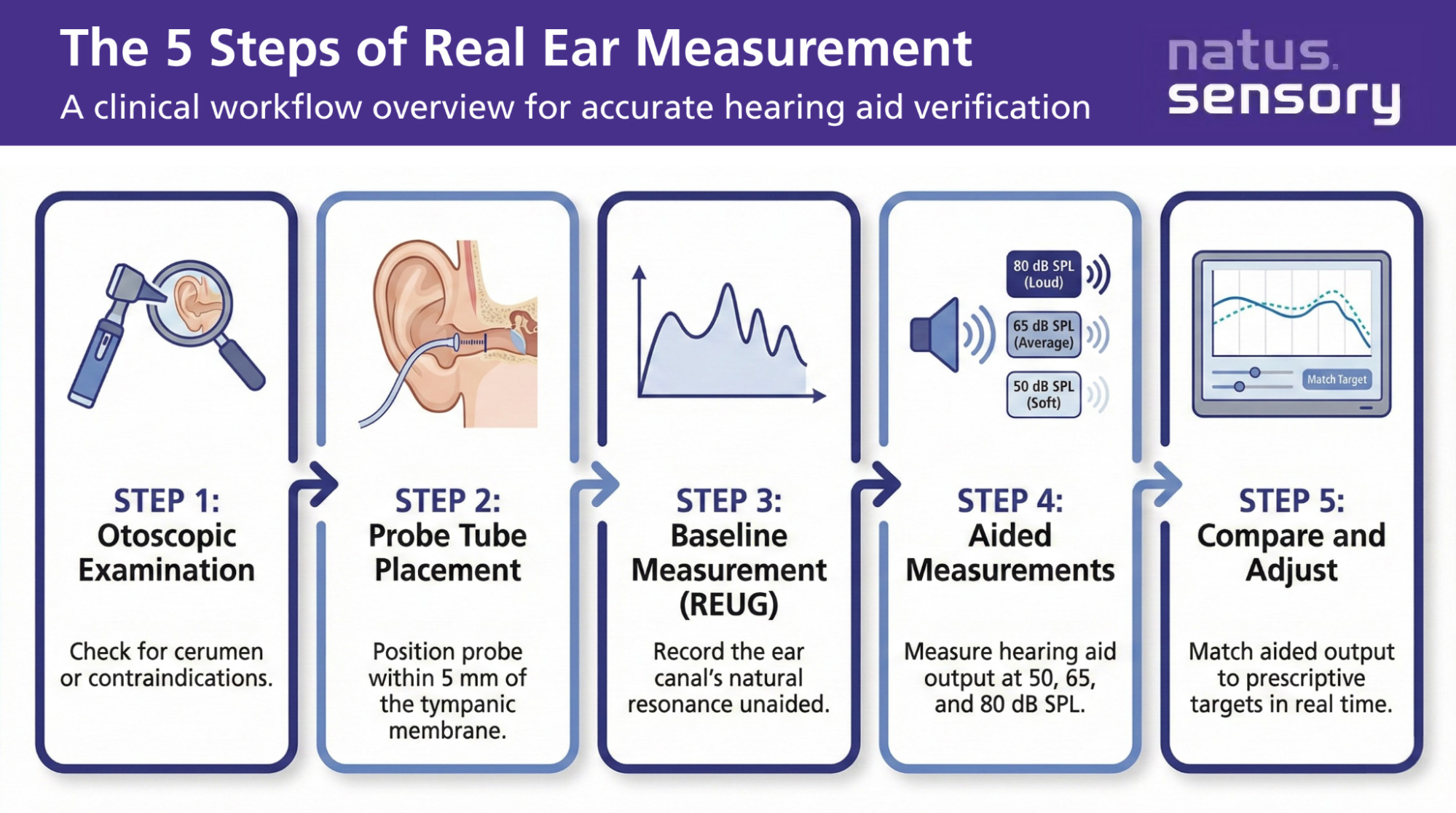
Step 1: Otoscopic Examination
Before probe tube placement, the hearing care provider examines the ear with an otoscope. This confirms there’s no excessive earwax or debris that could interfere with the measurement.
Step 2: Probe Tube Placement
A thin silicone probe tube is inserted into the patient’s ear canal, typically positioned within 5 mm of the tympanic membrane. Accurate probe tube placement is a must because the position of the tube directly affects the accuracy of the measurement.
Step 3: Baseline Measurement (REUG)
With the probe microphone in place and no hearing aid inserted, the clinician runs a Real Ear Unaided Gain (REUG) measurement. This captures how the patient’s ear canal naturally amplifies sound based on its unique shape and volume, documenting those individual differences.
Step 4: Aided Measurements
The hearing aid is inserted alongside the probe tube. The REM system then plays different sounds at multiple input levels:
The system records the hearing aid’s output at each level and displays it against the prescriptive target on screen.
Step 5: Adjustments and Verification
The audiologist makes real-time adjustments through the programming software until the hearing instrument’s output closely matches the target for each frequency and input level. The process also confirms that loud sounds stay within a comfortable range, protecting the patient from over-amplification.
| Test | What It Measures |
| REUG (Real Ear Unaided Gain) | The ear canal’s natural resonance without a hearing aid in place |
| REOG (Real Ear Occluded Gain) | The effect of the hearing aid shell or earmold in the ear with the device turned off; includes measure of the occluded ear |
| REAR (Real Ear Aided Response) | The actual sound level delivered by the hearing aid at the tympanic membrane |
| Speech Mapping | Uses speech or speech-like signals to show how the hearing aid processes real-world speech across frequencies |
The evidence supporting REM is clear. A systematic review and meta-analysis published in Trends in Hearing found that probe-tube verification of real ear hearing aid amplification improved self-perceived listening ability, communication outcomes, and understanding of speech in background noise.
Specific findings from current research include:
Fewer return visits, better speech clarity, and higher device retention rates all point to the value of including REM as a standard part of the hearing aid fitting process.
No two ear canals are the same. The length, diameter, and unique shape of each ear canal affect how sound travels to the tympanic membrane. Even a patient’s left and right ears will differ in their acoustic properties.
These physical differences mean that:
Real ear measurement accounts for all of these variables. It gives the clinician a window into what is actually happening at the eardrum, rather than relying on predictions based on population averages.
Speech mapping is a form of REM that uses real or recorded speech signals instead of pure tone beeps. It shows how the hearing aid processes actual speech patterns, giving clinicians and patients a visual representation of hearing aid performance across frequencies.
Why speech mapping is useful:
REM also allows clinicians to verify advanced features like noise reduction algorithms and directional microphones. Without real ear verification, there is no objective way to confirm these features are working as intended in the patient’s ear.
For the hearing aid user, real ear measurement is a quick and comfortable process. Most patients describe the probe tube as a slight tickle inside the ear. The entire process typically takes 10 to 15 minutes per ear.
During the appointment, patients can expect:
The process addresses each patient’s unique needs and gives the hearing care provider objective data to support the fitting.

Getting the Most from Every Hearing Aid Fitting
Real ear measurement gives clinicians the objective data they need to deliver personalized, evidence-based hearing aid fittings. By measuring the actual sound level inside a patient’s ear canal, REM accounts for individual differences in ear anatomy, verifies that amplification levels match prescriptive targets, and confirms that the hearing instrument is performing as intended.
Natus Sensory supports this best practice through the Aurical® portfolio of fitting systems, which integrates real ear measurement, verification, and counseling into a single workflow powered by Otosuite® software. These systems are designed with clinicians in mind, supporting accurate, repeatable fittings that improve patient outcomes. To learn more about how Natus Sensory’s hearing aid fitting solutions can support your clinic, contact us today.
Sources:
053103 RevA